








{kind=link}
-
Purpose:
To describe the clinical findings and diagnostic approach of a patient diagnosed with Vogt Koyanagui Harada disease initially studied for suspected optic neuritis.
-
Case Report:
A 30 year-old female patient with initial suspicion of optic neuritis reported hearing loss and tinnitus of 1 year of evolution, in addition to arthralgia in the metacarpals and pain in the lumbar region. Her visual acuity in the right eye was counting fingers at 3 meters and 20/400 in the LE. Few fine retrokeratic precipitates were found, minimal cellularity in anterior chamber and pigment in the anterior lens capsule; ++ vitreous cellularity, optic nerve with blurred edges, multiple hypopigmented placoid lesions, multiple areas of serous detachments, peripheral snowballs. In the OCTA, marked vitreitis was found with loss of retinal architecture secondary to multiple serous retinal detachments and thickened choroid in both eyes. In the OCT of the NFL, thickening of the NFL was documented. Given the clinical and imaging findings, it was considered that the patient has Vogt Koyanagui Harada disease, so application of sub-tenon triamcinolone 20 mg was recommended in BE, achieving visual acuity in the right eye of 20/150 and the left eye of 20/150 with significant decrease of inflammatory reaction and serous detachments.
-
Discussion:
Vogt Koyanagui-Harada disease is an flammatory disease capable of causing neurologic, ocular, and cutaneous symptoms.
The disease primarily affects races with darker pigmentation
There is no sex predilection.
VKH has been found to be linked with human leukocyte antigen.
The course of VKH includes three phases: acute, convales- cent, and chronic phases.
The presentation of VKH usually starts with headache, associated with red eye, blurred vision, tinnitus, and vertigo.
In mild form, the vitreous cells are scanty; only mild choroidal folds with slightly hyperemic disc may be seen with headache along with disc edema and mild pleocytosis in cerebral spinal fluid.
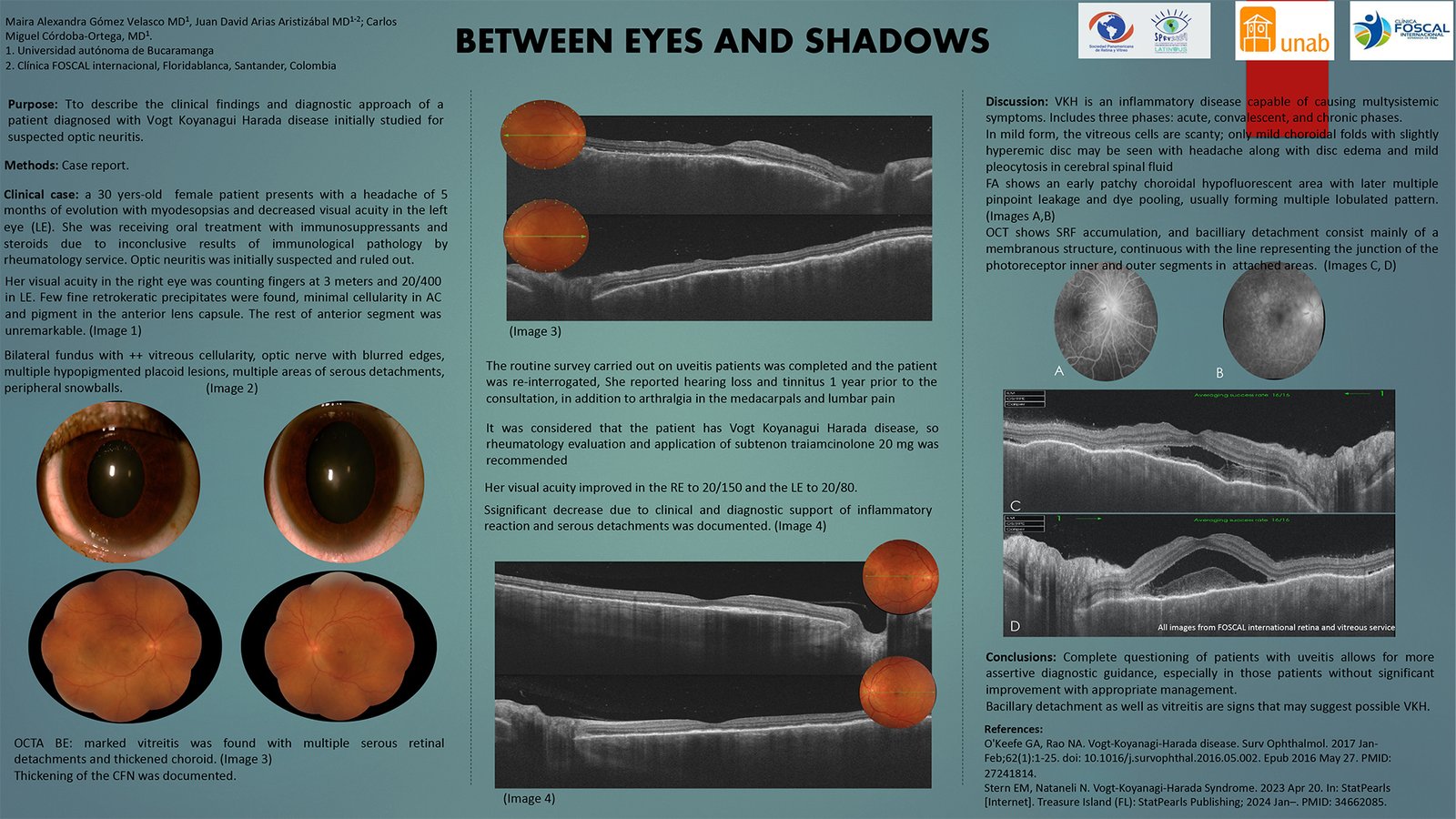
Fluorescein angiography shows an early patchy choroidal hypofluorescent area with later multiple pinpoint leakage and dye pooling, usually forming multiple lobulated pattern.
In the OCT in addition to the usual pattern of SRF accumulation, the floors of the bacilliary detachment consist mainly of a membranous structure, continuous with the line representing the junction of the photoreceptor inner and outer segments in attached areas.
The treatment of choice in acute stage is high-dose corticosteroid.
In severe cases of VKH, immunosuppressive treatment may be needed.
The prognosis is usually good unless there is chronic inflamma- tion or choroidal neovascularization.
Our patient debuted with a diagnosis of optic neuritis; However, the clinical and imaging characteristics guide the diagnosis towards VKH. Given the multiple forms of presentation and differential diagnoses, complete questioning and multimodal imaging of patients with uveitis can guide the diagnosis and allow timely treatment. -
Conclusions:
Complete questioning of patients with uveitis allows for more assertive diagnostic guidance, especially in those patients without significant improvement with appropriate management.